
What Are the Symptoms of C-PTSD After Narcissistic Abuse?

If you have survived a relationship with a narcissist, you know the aftermath isn’t just heartbreak; it feels like a fundamental rewiring of who you are.
While standard trauma frameworks often fail to capture this specific brand of psychological erosion, thousands of survivors find themselves battling a distinct, severe echo of their past: the debilitating symptoms of C-PTSD after narcissistic abuse.
Unlike traditional post-traumatic stress, which typically stems from a single, shocking event, Complex PTSD is the direct result of prolonged, relational captivity where your reality was systematically dismantled.
If you are currently dealing with severe emotional volatility, an inner critic that sounds exactly like your abuser, or a nervous system that refuses to exit survival mode, you aren’t “crazy,” and you aren’t failing to heal.
You are experiencing the predictable physical and psychological hallmarks of long-term interpersonal trauma.
Understanding how these symptoms manifest in your body, mind, and relationships is the critical first step toward breaking the invisible trauma bonds and reclaiming your stolen identity.
- C-PTSD represents a distinct diagnosis from PTSD. It includes three additional symptom clusters beyond standard trauma responses.
- Narcissistic abuse causes C-PTSD because the experience is prolonged and interpersonal. It specifically targets your identity and your sense of reality.
- Symptoms appear emotionally through dysregulation and shame. You notice them relationally through distrust and isolation. You feel them physically through exhaustion and nervous system dysregulation.
- Recovery happens when you use the correct approach. You address both the cognitive and body-based dimensions of your trauma.
What Is C-PTSD and How Is It Different from PTSD?
To understand Complex Post-Traumatic Stress Disorder (C-PTSD), we have to look past standard clinical definitions and examine the architecture of trauma itself.
Standard PTSD is typically born from a discrete, time-bound shock, a car accident, a natural disaster, or a singular violent event. The brain flags that specific moment as dangerous, and the survival system tries to avoid reminders of it.
C-PTSD is entirely different. It is the psychological and physiological blueprint left behind by prolonged, repetitive interpersonal trauma from which escape feels impossible.

Recognizing this diagnostic gap, the World Health Organization formally included C-PTSD in the ICD-11 classification system in 2022.
While it was famously omitted from the DSM-5 because 95% of diagnostics overlapped with standard trauma criteria, clinicians worldwide recognized that treating a survivor of relational captivity required a radically different map.
To be diagnosed with C-PTSD, you must meet the core criteria of traditional PTSD:
C-PTSD introduces three additional symptom clusters that fundamentally alter a survivor’s internal landscape. These are not just extra symptoms; they represent a severe disturbance in “Disturbances in Self-Organization” (DSO):
The Three Additional Clusters of C-PTSD
| Symptom Cluster | Standard Definition | The Reality (Lived Experience) |
|---|---|---|
| Severe Emotional Dysregulation | “Swinging from explosive rage to numb detachment.” | Your brain’s volume knob breaks. Unpredictable abuse strips your nervous system of the ability to smoothly transition between emotions. You find yourself trapped in either an active state of terror or a frozen state of blankness. |
| Pervasive Negative Self-Beliefs | “Carrying a sense of shame, guilt, and worthlessness.” | You develop a structural conviction regarding your defectiveness rather than simple low self-esteem. You internalize the constant projections of the abuser. Your inner dialogue shifts from “I receive poor treatment” to “I possess brokenness.” |
| Persistent Relational Difficulties | “Finding trust dangerous or difficult.” | You experience hyper-vigilance toward interpersonal cues. Your brain learns to read micro-expressions as existential threats. A slight shift in a partner’s tone triggers a full physical panic response because your brain assumes punishment approaches. |
Complex trauma is far more prevalent than public awareness suggests. While C-PTSD affects approximately 4% of the general population, that number explodes to 15% in cohorts exposed to prolonged domestic or psychological captivity.
If you are experiencing these extra layers, you aren’t suffering from a standard fear response; you are navigating a systematically fractured sense of self.

Why Does Narcissistic Abuse Cause C-PTSD Specifically?
Not all prolonged trauma produces Complex PTSD. While surviving a war zone or a natural disaster can shatter a person’s sense of safety, the specific nature of narcissistic abuse acts as a targeted strike against the survivor’s psychological core.
To understand why this environment is uniquely fertile ground for C-PTSD, we have to look at the intersection of evolutionary biology and deliberate psychological manipulation.
Narcissistic abuse is interpersonal at its core. It happens within a relationship, romantic, familial, or professional- that was supposed to be safe.
When the primary source of danger in your life is simultaneously the primary source of your validation and comfort, the brain faces a catastrophic paradox.
The Psychology of Betrayal Trauma
To explain this entrapment, psychologists point to the framework of Betrayal Trauma. Human beings are wired for attachment; it is an evolutionary survival mechanism.
When an individual is dependent on an abuser for emotional survival, financial stability, or social cohesion, the brain executes a survival strategy called betrayal blindness.
The brain purposefully suppresses awareness of the abuse to preserve the critical attachment bond. You do not stay because you are weak; your brain actively rewires your perception to tolerate the intolerable because it views isolation as an existential threat.
This survival mechanism is further locked in place by a predictable, destructive cycle:
┌────────────────────────────────────────┐
▼ │
[Idealization] ──► [Devaluation] ──► [Discard & Vacuum]
The Neurochemical Cage of Intermittent Reinforcement
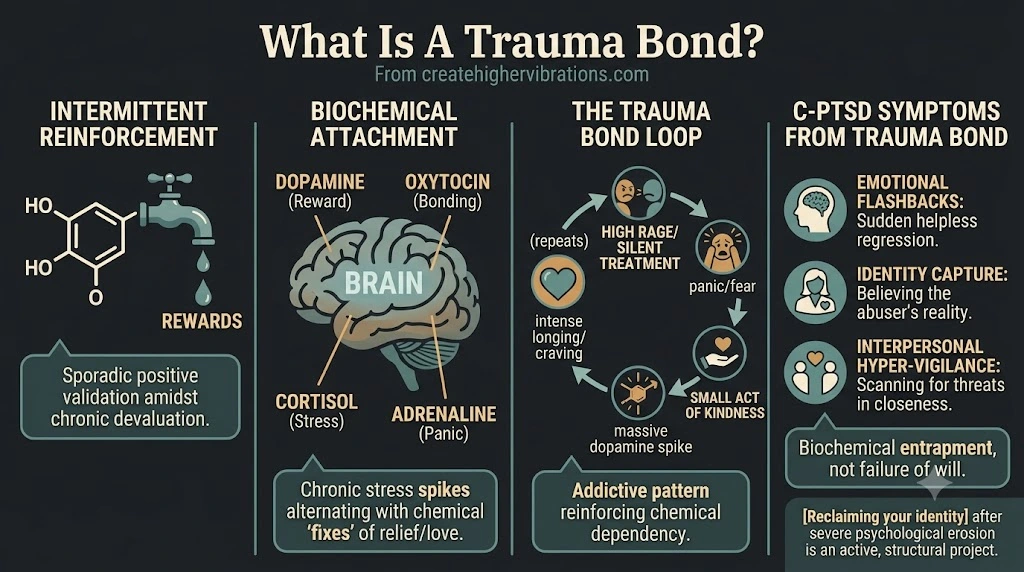
Each round of this cycle reinforces the trauma bond through the same biochemical mechanisms that drive substance addiction.
If an abuser were cruel 100% of the time, the defense systems of the brain would choose flight or fight.
But narcissistic abuse relies heavily on intermittent reinforcement, the psychological phenomenon where rewards are delivered unpredictably.
During the idealization or “love-bombing” phases, your brain is flooded with dopamine (the reward chemical) and oxytocin (the bonding hormone).
When the abuse shifts into devaluation, your system drops into a cortisol-and-adrenaline-fueled panic.
┌────────────────────────────────────────────────────────┐
│ THE BIOCHEMICAL TRAUMA BOND COIL │
├───────────────────────────┬────────────────────────────┤
│ Abuser's Action │ Neurochemical Release │
├───────────────────────────┼────────────────────────────┤
│ Love-Bombing/Validation │ ✦ Dopamine & Oxytocin │
│ │ (High Euphoria & Bond) │
├───────────────────────────┼────────────────────────────┤
│ Devaluation/Gaslighting │ ▲ Cortisol & Adrenaline │
│ │ (High Panic & Anxiety) │
└───────────────────────────┴────────────────────────────┘
When the abuser suddenly throws a crumb of warmth or validation after a period of cruelty, the relief triggers a massive, unnatural spike in dopamine. This neurochemical rollercoaster creates a profound, physiological craving.
You become chemically dependent on the person causing your distress, rendering the toxic effects of narcissistic abuse structurally indistinguishable from a severe drug dependency.
The Systematic Erasure of Reality
Beyond the biochemical cage, the damage of these abuse patterns strikes directly at your cognitive operating system. A narcissist does not simply mistreat you; they systematically replace your sense of reality with their own via chronic gaslighting and projection.
When you are repeatedly told that your perceptions are flawed, your boundaries are “attacks,” and your memories are fabricated, your brain eventually stops trying to reconcile the contradiction. To maintain the relationship, you cede your critical thinking over to the abuser.
This systematic erasure is precisely what forms the “Pervasive Negative Self-Beliefs” cluster of C-PTSD. It is why, long after you leave the physical environment, your internal dialogue continues to echo the voice of your abuser. Your identity wasn’t just damaged; it was overwritten.

What Are the Emotional Symptoms of C-PTSD After Narcissistic Abuse?
The emotional symptoms of C-PTSD are often the most debilitating because they feel entirely voluntary-resistant. Survivors frequently present to therapy believing they have developed a mood disorder like Bipolar or Borderline Personality Disorder.
In reality, what looks like psychiatric instability is actually the structural footprint of a nervous system that has been forcefully reorganized by prolonged trauma.
When you survive chronic interpersonal abuse, your brain’s fear center, the amygdala, becomes permanently hyperactive. It loses its ability to accurately distinguish between a past existential threat and a present, neutral interaction.
The Phenomenon of Emotional Flashbacks
The most insidious manifestation of this hyperactive threat system is the emotional flashback. Unlike classical PTSD flashbacks, which are typically visual or auditory (e.g., a combat veteran seeing or hearing a battlefield), a C-PTSD flashback is purely affective.
You do not see a memory; you feel it.
During an emotional flashback, a minor present-day trigger causes you to instantly regress into the exact emotional state you occupied during the worst periods of the abuse. Suddenly, without warning, you are consumed by intense waves of:
Because there is no visual component to guide your logic, your brain assumes this intense emotional reaction is being caused by whatever is happening right now.
If a partner sighs or a boss sends a vague text, you don’t just feel minor worry; you plunge into the terrifying depth of a trauma response, completely unmoored from the present context.
Subscribe to Create Higher Vibrations!
Get Inspiration and Practical advice straight to your inbox.
Structural Dissociation: The Broken Volume Knob
This chronic threat activation shatters your capacity for emotional regulation. Your brain’s “volume knob” is broken, causing you to bounce between two extreme states of the autonomic nervous system:
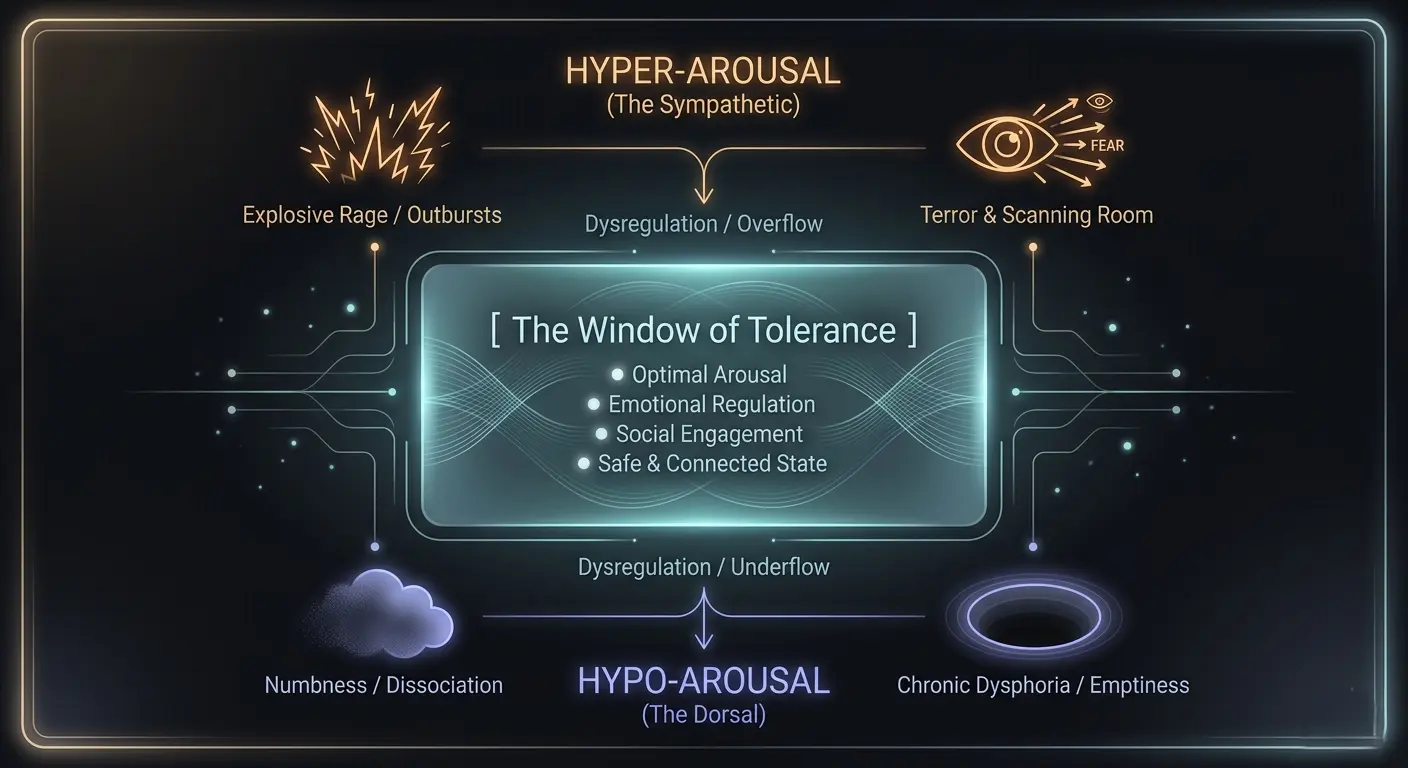
You are either trapped in hyperarousal (panic, intense emotional triggers, or sudden bursts of protective rage) or you violently crash into hypoarousal. The dorsal vagal pathway governs this survival state.
It manifests as a profound, protective numbness, a state of “freeze or collapse” where you feel utterly detached from your body, your environment, and your capacity to feel joy.
The Spiritual Collapse: Alterations in Systems of Meaning
The final, deeply hidden emotional symptom of C-PTSD is what the ICD-11 classifies as alterations in systems of meaning. Narcissistic abuse does not just change how you feel; it damages your existential framework.
When a person who claims to love you systematically devalues you, it fractures your fundamental assumptions about human nature, safety, and justice. This often leads to persistent dysphoria, a low-grade, chronic sense of hopelessness.
Survivors frequently report a total loss of faith in spiritual frameworks, an overwhelming sense that the universe is inherently hostile or indifferent, and a deep, agonizing belief that a normal, peaceful life is forever out of reach for them.
Learning to identify your emotional triggers is an important part of recovery. Understanding that these triggers are symptoms of C-PTSD, not evidence of personal failure, is what makes healing possible.
How Does C-PTSD Affect Your Sense of Self and Identity?
Of all the complex trauma clusters, identity erosion is often the most agonizing. Narcissistic abuse does not merely damage your self-esteem; it systematically dismantles your self-concept.
While standard domestic friction might leave you feeling unappreciated, chronic narcissistic manipulation leaves you asking a far more terrifying question: “Who am I when no one is watching?”
This erasure of identity happens slowly, over months or years of your perceptions being rewritten and your boundaries being treated as acts of aggression. The abuser does not simply criticize your behavior; they attack your fundamental worth as a person.
The Split: Ordinary Shame vs. C-PTSD Toxic Shame
To understand the mechanics of this erosion, we must differentiate between two very different internal experiences:
The Neuroscience of Fractured Identity
This loss of self is not an imaginary emotional state; it is a documented neurological event.
Modern neuroimaging reveals that chronic trauma completely disrupts the Default Mode Network (DMN), the interconnected brain regions responsible for generating your baseline sense of self, autobiographical memory, and self-reflection.
When you are constantly adapting to an unpredictable, hostile partner, your prefrontal cortex dials down its activity to prioritize immediate survival.
The DMN is hijacked. Your brain stops tracking your desires, your preferences, and your organic personality because doing so is dangerous.
To survive, you must become hyper-focused on the abuser’s emotional state. Your internal operating system swaps out your authentic self-concept for a fragmented, hyper-vigilant adaptation designed solely to minimize conflict.
The Symptoms of a Fragmented Self-Concept
When you finally escape the relationship, this neurological adaptation manifests as a deeply unsettling psychological void. Survivors frequently report a distinct set of identity-based symptoms:
Reclaiming your identity after this level of psychological erosion is not about “finding” an old version of yourself.
It is an active, structural project of dismantling the false, survival-driven self the abuser forced you to construct, and safely giving your nervous system permission to build a new one from the ground up.

Why Do Relationships Feel Impossible After Narcissistic Abuse?
The relational fallout of complex trauma is often the most isolating symptom of the disorder.
Survivors frequently escape an abusive environment expecting immediate relief, only to find that their ability to connect with, trust, and feel safe around other human beings has been completely compromised.
This happens because your survival system treats the end of the abuse as a geographical change, not a physiological one.
When a person you loved used your vulnerability as a psychological weapon, your nervous system learned a devastating survival rule: Closeness equals danger.
The Breakdown of Trust and Interpersonal Hyper-vigilance
When you enter a new, healthy relationship after surviving a narcissist, your hyper-vigilant threat detection system goes into overdrive.
Because you were chronically blindsided by an abuser who masked micro-aggressions behind a smile, your brain can no longer accept kindness at face value.
When you meet someone genuinely kind, your nervous system interprets their consistency as a trap or a calculations-based manipulation.
This triggers a profound internal panic, often causing survivors to prematurely sabotage connections or push safe people away as an act of pre-emptive self-defense.
The Trauma Repetition Loop and Perpetrator Preoccupation
The ICD-11 specifically highlights that the relational cluster of C-PTSD manifests through highly distinct behavioral patterns. Rather than simply avoiding people, survivors often find themselves trapped in two deeply painful, paradoxical dynamics:
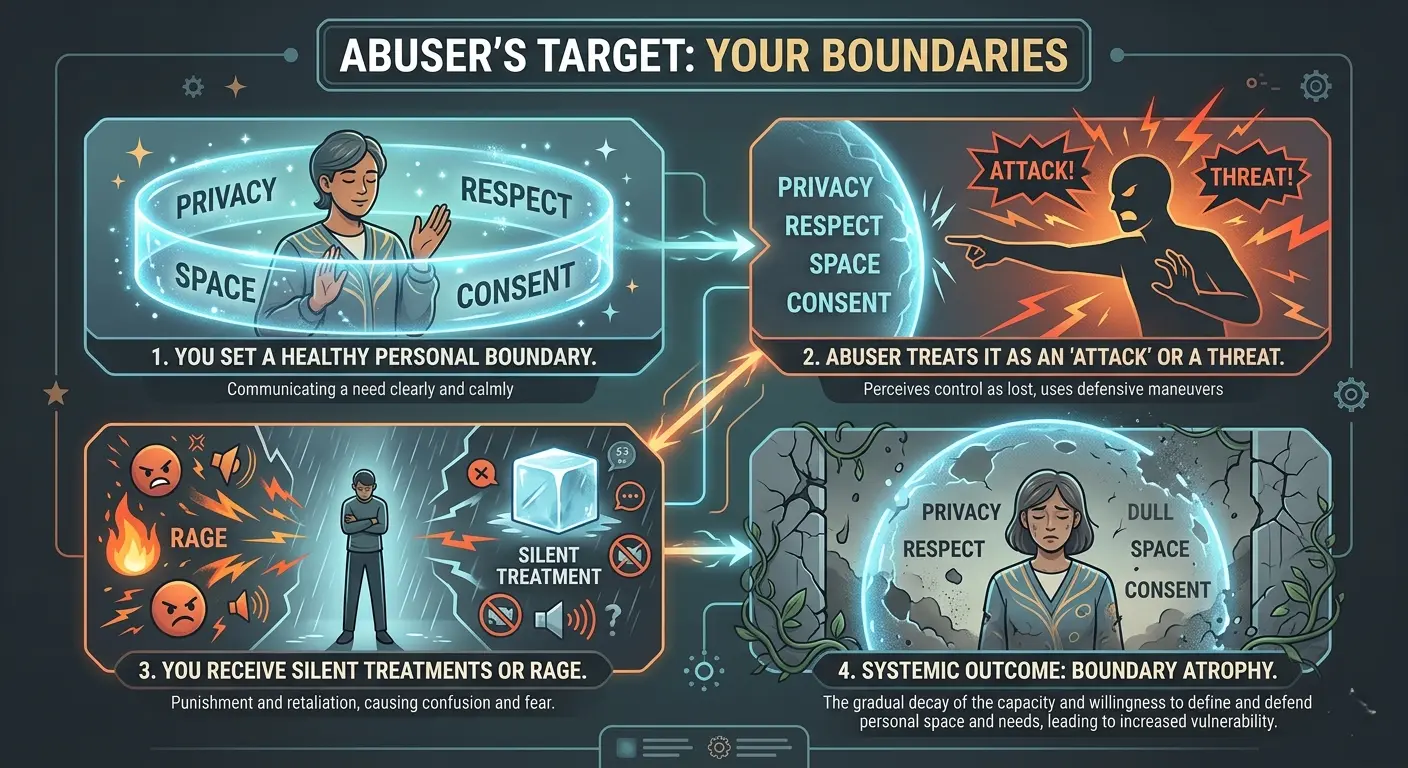
The Atrophy of Self-Protection
The reason these relational patterns repeat is that your boundary-setting apparatus was intentionally dismantled during the abuse.
Setting boundaries after narcissistic abuse feels terrifying because, in your past, a boundary was treated as an act of war, resulting in severe punishment, silent treatments, or raging devaluations.
You are not suffering from a personal failure of will; you are suffering from a predictable, structural consequence of relational captivity.
Healing this cluster does not happen by forcing yourself to blindly trust others; it happens by slowly rebuilding your capacity to trust yourself to spot red flags, enforce consequences, and safely exit spaces that echo your past.
What Is the Trauma Bond and Why Does It Keep Pulling You Back?
The trauma bond is arguably the most misunderstood aspect of narcissistic abuse. Friends, family, and even untrained clinicians will often look at a survivor and ask, “If they were so cruel, why do you miss them?”
This question betrays a fundamental ignorance of trauma biology. A trauma bond is not a reflection of codependency, a lack of willpower, or lingering love.
It is a state of severe, involuntary biochemical entrapment.
The Agony of Neurochemical Withdrawal
When you finally leave a narcissistic relationship, your brain does not celebrate freedom; it enters a state of acute, clinical withdrawal structurally identical to detoxing from an opioid addiction.
During the relationship, the abuser’s cycle of unexpected cruelty and sporadic love-bombing functioned as an unpredictable drug dispensary.
THE COGNITIVE & CHEMICAL WITHDRAWAL LOOP
┌──────────────────────────────────────────────┐
│ 1. Physical Separation From the Narcissist │
├──────────────────────────────────────────────┤
│ 2. Massive Drop in Dopamine & Oxytocin │
├──────────────────────────────────────────────┤
│ 3. Amygdala Screams: "Existential Danger!" │
├──────────────────────────────────────────────┤
│ 4. Intense Craving / Obsessive Scanning │
└──────────────────────────────────────────────┘
The moment you break contact, your brain experiences a catastrophic drop in dopamine and oxytocin, while your stress hormones (cortisol and adrenaline) spike. This chemical deficit tricks your survival brain into believing you are in existential danger.
Your obsessive tracking of their social media, your impulse to text them, and the painful physical emptiness in your chest are your brain’s frantic attempts to get a “fix” of the abuser to regulate your agonizing internal state.
Paradoxical Gratitude and Identity Capture
As pioneering traumatologist Judith Herman established in her foundational text, Trauma and Recovery, prolonged captivity forces the human psyche to develop a “supernatural relationship” with the abuser.
When an abuser controls your access to emotional safety, basic validation, or peace, your brain stops viewing them as an enemy and begins viewing them as a godlike arbiter of your survival.
This psychological adaptation leads to two core symptoms of C-PTSD identified in the ICD-11:
Breaking a trauma bonding loop requires treating yourself not as a failed partner, but as a recovering addict. Healing does not begin when the cravings stop; it begins when you learn to sit through the chemical withdrawal without breaking No Contact.
How Does C-PTSD Show Up in Your Body?
Many survivors spend years attempting to think their way out of trauma using cognitive talk therapies, only to find their physical health completely deteriorating.
This is because C-PTSD is fundamentally a body-based disorder. As Dr. Bessel van der Kolk famously detailed, trauma is stored in the nervous system and deep somatic tissues, completely bypassing the logical brain.
When you endure months or years of chronic relational stress, your body’s baseline calibration is forced to shift. The constant, toxic flood of cortisol and adrenaline eventually wreaks havoc on your physical biology, turning psychological terror into physiological illness.
The Autonomic Trap: Polyvagal Theory
To understand why your body feels ruined after narcissistic abuse, we must look at the Polyvagal Theory, pioneered by Dr. Stephen Porges.
A healthy nervous system operates within a “Social Engagement System,” where it can easily switch between minor stress and deep relaxation.
Complex trauma destroys this flexibility, locking your body into a permanent survival loop between two hostile branches of the autonomic nervous system:
Somatization and Systemic Inflammation
This constant autonomic whiplash causes severe somatization, the conversion of unexpressed psychological terror into chronic physical illness.
The vagus nerve, which regulates your heart rate, lungs, and digestive tract, becomes deeply dysregulated.
┌────────────────────────────────────────────────────────┐
│ THE PHYSIOLOGICAL FOOTPRINT OF C-PTSD │
├───────────────────────────┬────────────────────────────┤
│ Vagal Target Organs │ Somatic Symptom │
├───────────────────────────┼────────────────────────────┤
│ Gastrointestinal System │ IBS, Leaky Gut, Reflux │
├───────────────────────────┼────────────────────────────┤
│ Immune System Response │ Autoimmune Flare-ups │
├───────────────────────────┼────────────────────────────┤
│ Musculoskeletal System │ Fibromyalgia, Migraines │
└───────────────────────────┴────────────────────────────┘
Because 90% of your body’s serotonin is produced in the gut, this vagal shutdown directly causes severe gastrointestinal conditions like Irritable Bowel Syndrome (IBS), food intolerances, and chronic acid reflux.
Prolonged cortisol saturation eventually triggers a systemic inflammatory response, causing the immune system to mistakenly attack its own tissues, explaining the massive statistical link between narcissistic abuse survivors and the onset of autoimmune disorders or fibromyalgia.
Since trauma is physically stored within your body’s tissues, intellectual methods like cognitive behavioral therapy are inherently inadequate when used in isolation.
True recovery demands the integration of bottom-up strategies, employing specific somatic exercises and body-oriented practices to securely release the survival energy stored in your nervous system.
What Are the Lesser-Known Symptoms People Miss?
When public discussions center around the effects of narcissistic abuse, they almost exclusively focus on emotional distress, crying spells, or overt trust issues. Complex PTSD is a systemic condition that quietly rewires your cognitive architecture.
Many survivors live with secondary, deeply disorienting symptoms for years without ever realizing they are direct neurological adaptations to prolonged trauma.
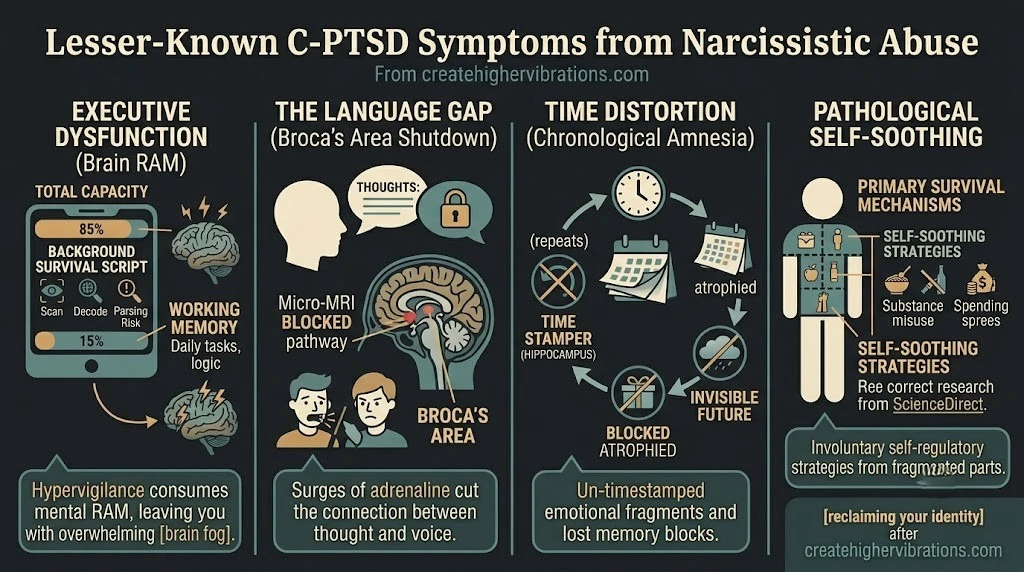
1. Executive Dysfunction and Cognitive Load Theory
Survivors frequently find themselves struggling to plan dinner, organize a basic schedule, initiate simple tasks, or maintain concentration.
This is not a character flaw, laziness, or early-onset cognitive decline. To understand this paralysis, we must look at Cognitive Load Theory.
Your brain possesses a restricted supply of working memory at any specific time. In a healthy state, that mental energy is available to navigate everyday life.
However, with C-PTSD, an overactive amygdala compels the brain to perpetually execute a heavy, underlying “survival script.” Your subconscious interprets tranquility as a logic error, meaning it refuses to lower its defenses.
TOTAL COGNITIVE BRAIN CAPACITY
┌────────────────────────────────────────────────────────┐
│ ░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░░ │
│ ▲ SYSTEM BACKGROUND TRAUMA LOADING (85%) │
│ (Scanning environment, decoding tones, parsing risk) │
├───────────────────────────────┬────────────────────────┤
│ █ ██ ██ ██ │ │
│ ▲ Working Memory Left (15%) │ ◄ Paralysis / Fog │
│ (Daily tasks, focus, logic) │ │
└───────────────────────────────┴────────────────────────┘
Your brain is continuously consuming its baseline fuel to scan your current environment, decode minor vocal tones, parse hidden threats, and manage the internal echo of the abuser’s voice.
Because your processing system is chronically running at 85% capacity to keep you upright, your executive function is starved of resources.
The result is an overwhelming, impenetrable brain fog and an involuntary shutdown of your task-initiation muscles.
2. The Language Gap: Broca’s Area Suppression
A highly specific and deeply frustrating symptom of relational trauma is a sudden, physical difficulty with communication.
Survivors often describe an agonizing gap between understanding a concept in their head and physically articulating those thoughts into spoken words, especially during moments of conflict or emotional arousal.
Neuroimaging studies explain this through the mechanics of the speech center of the brain.
When a trauma trigger activates your nervous system, the intense surge of adrenaline causing your panic simultaneously suppresses Broca’s area, the region of the left prefrontal cortex solely responsible for translating thoughts into articulated speech.
When you were undergoing chronic abuse patterns, speaking up or defending yourself resulted in immediate retaliation. Your brain learned that verbal self-defense was fundamentally unsafe.
Over time, your system optimized its survival by physically cutting the connection between your thoughts and your voice, causing you to literally go mute or stammer when your survival system feels threatened.
3. Chronological Amnesia and Time Distortion
Trauma completely disrupts the brain’s ability to linearize data. The hippocampus, which acts as the brain’s internal time-stamper, atrophies under chronic cortisol exposure.
Consequently, your memories are not stored as orderly historical files; they are stored as raw, un-timestamped emotional fragments. This causes profound time distortion:
4. Pathological Self-Soothing and Secondary Structural Dissociation
Finally, survivors often battle intense guilt over hidden behavioral patterns like compulsive eating, sudden hyper-frugality, substance misuse, or erratic spending sprees.
It is vital to understand these behaviors through the lens of Secondary Structural Dissociation.
Such behaviors are not character flaws or signs of insufficient willpower. They are raw, frantic coping mechanisms employed by lonely, wounded facets of your identity attempting to force a neurochemical boost into a collapsing, over-governed system.
According to research published on ScienceDirect, anywhere from 28.6% to 76.9% of individuals with C-PTSD navigate significant clinical dissociation.
Even if you do not experience full visual or environmental detachment, your brain will compartmentalize your personality into distinct parts: a “functional part” that goes to work and pays bills, and a “traumatized part” that carries the agonizing weight of the abuse.
Bridging this internal divide requires moving past self-condemnation and recognizing that every single one of your confusing symptoms was once an elegant, highly successful strategy designed to keep you alive.
How Is C-PTSD From Narcissistic Abuse Treated?
Recovering from Complex PTSD requires a radical departure from standard psychiatric protocols. Traditional, “top-down” approaches like Cognitive Behavioral Therapy (CBT), which focus on challenging and restructuring thoughts, are notoriously ineffective when used in isolation for this population.
Survivors of narcissistic abuse are usually highly intellectualized; they can analyze their abuse with clinical precision, yet their bodies remain trapped in a perpetual fight, flight, or freeze loop.
Because trauma physically alters the nervous system, you cannot talk your way out of a somatic survival response.
The Foundational Map: Herman’s Three-Stage Recovery Model
To safely navigate healing without triggering severe emotional destabilization, clinical consensus relies on the phase-based model pioneered by Dr. Judith Herman in Trauma and Recovery.
THE PHASE-BASED HEALING ROADMAP
┌──────────────────────────────────────────────┐
│ Phase 1: Establishing Safety & Regulation │
├──────────────────────────────────────────────┤
│ Phase 2: Remembrance, Mourning & Processing │
├──────────────────────────────────────────────┤
│ Phase 3: Reconnection & Identity Creation │
└──────────────────────────────────────────────┘
Phase 1: Safety and Stabilization (Bottom-Up Regulation)
Before a survivor can safely look at their memories, they must establish physical and environmental safety.
This means enforcing absolute No Contact with the abuser, establishing a stable routine, and learning to widen their nervous system’s window of tolerance.
Therapies like Dialectical Behavior Therapy (DBT) are highly effective here for building immediate distress tolerance skills, alongside targeted somatic exercises to soothe a hyperactive amygdala.
Phase 2: Remembrance and Mourning (Trauma Processing)
Once the nervous system is no longer operating in an acute crisis state, processing can begin.
This phase involves desensitizing the raw, un-timestamped emotional fragments stored in the brain and grieving the systematic theft of your time, reality, and identity.
Phase 3: Reconnection (Reclaiming the Self)
The final stage is existential. It involves stepping out of the survivor identity and actively designing a new life.
Here, the focus shifts to practicing healthy setting boundaries, overcoming interpersonal hypervigilance, and embarking on the profound project of reclaiming your identity from the ground up.
The Ultimate “Bottom-Up” Modality Toolkit
If you are seeking a trauma-informed practitioner to guide your healing journey, prioritize therapists certified in modalities that target the subcortical brain and autonomic nervous system:
| Modality | How It Works | Target Symptom |
|---|---|---|
| Somatic Experiencing (SE) | Tracks physical sensations in your body to safely discharge trapped fight or flight energy. | Chronic fatigue, muscle bracing, and irritable bowel syndrome. |
| Sensorimotor Psychotherapy | Integrates body awareness with meaningful psychological processing. | Postural collapse and structural numbness. |
| Trauma-Sensitive Yoga | Uses gentle movement to restore your sense of physical ownership and control. | Dissociation and looking-glass emptiness. |
The baseline truth of complex trauma recovery is simple: your body spent years modifying its shape, chemistry, and cognitive load to keep you alive inside an active war zone.
Healing isn’t about rushing to fix your symptoms; it is about building enough systemic safety so your nervous system can finally decode that the war is over.
Final Thought
Understanding your symptoms is not about labeling yourself. It is about making sense of an experience that was designed to make no sense.
C-PTSD after narcissistic abuse is a normal response to an abnormal situation. Your symptoms are not evidence that you are broken. They are evidence that you survived.
Healing is not linear. It requires honesty about what happened, patience with yourself as you process it, and willingness to accept support. You do not have to do this alone.

